2022 Plan Rates
Medical Rates
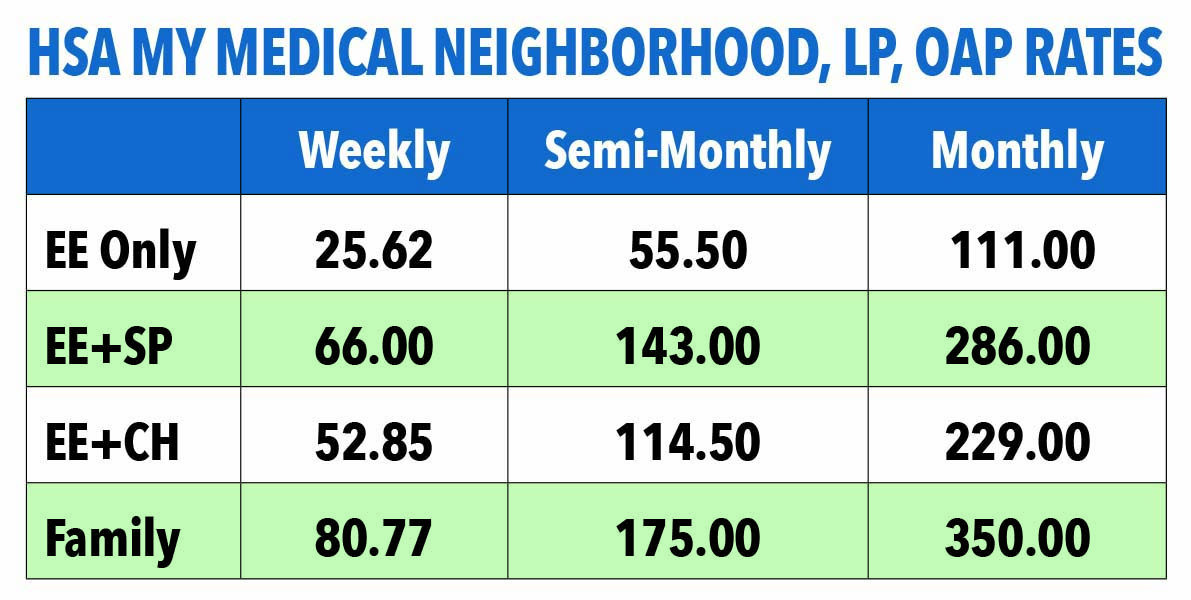
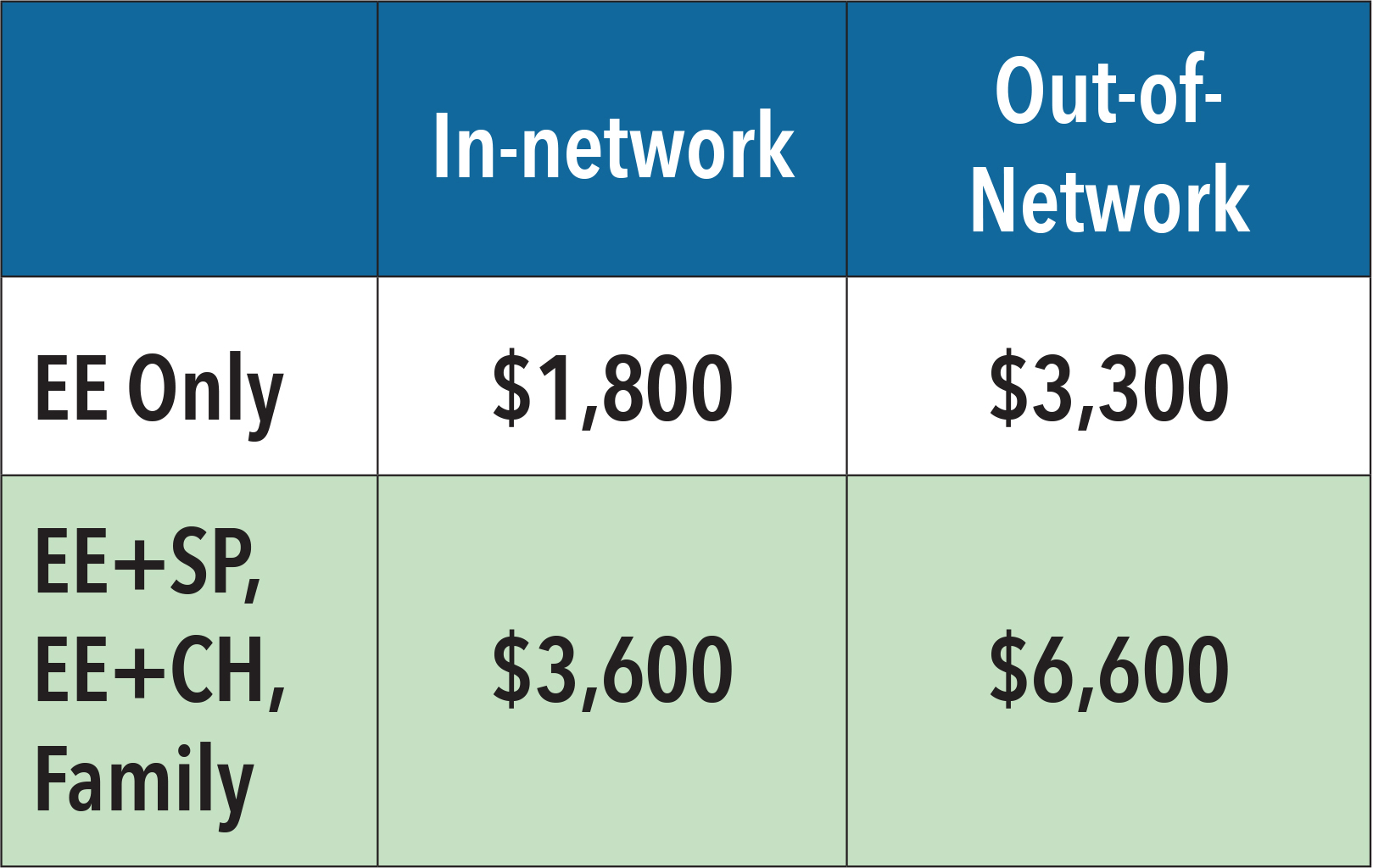
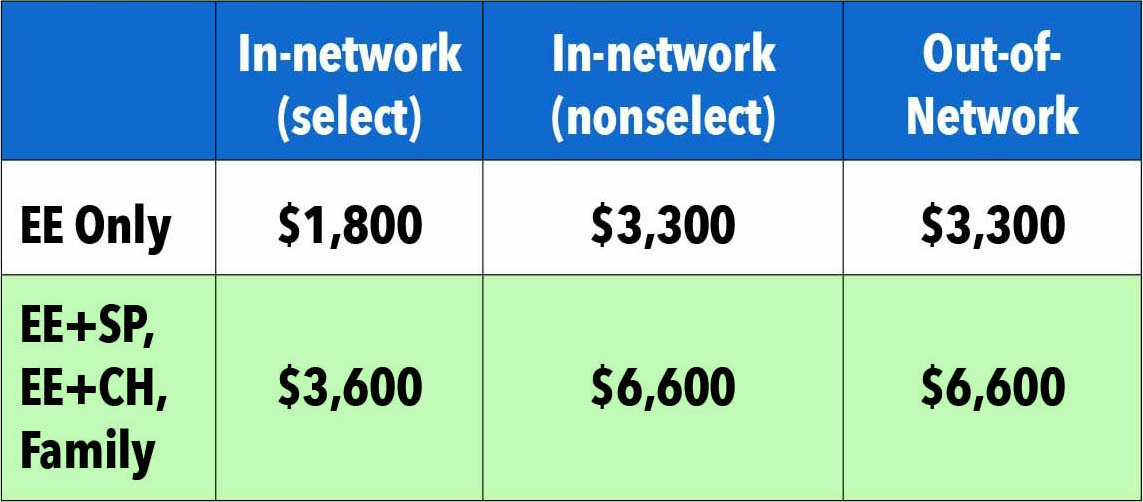
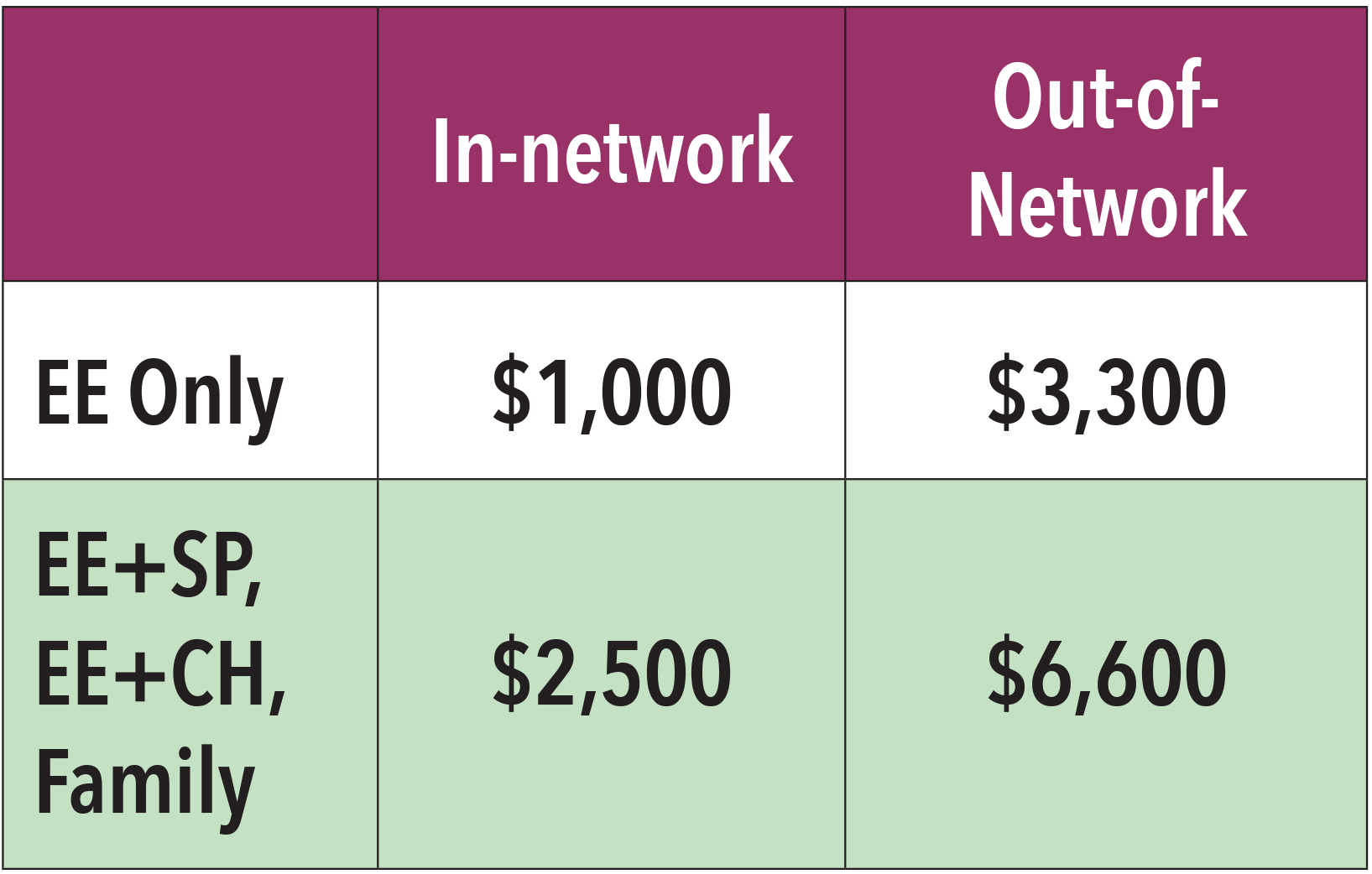
HSA PLANS
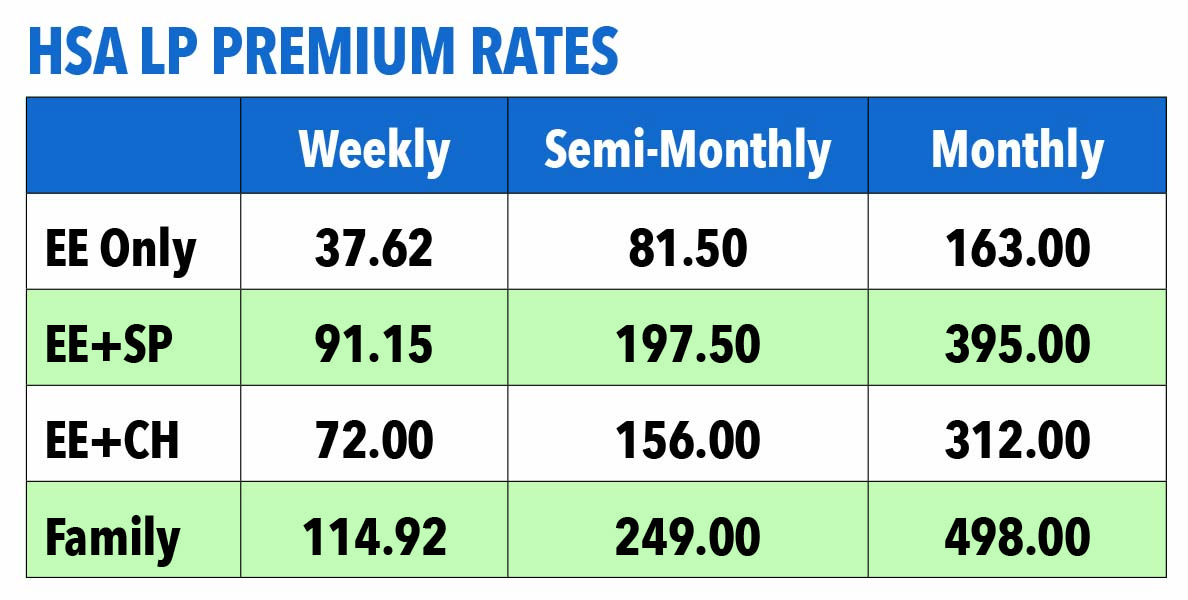
Deductibles
|
|
|
 |
 |
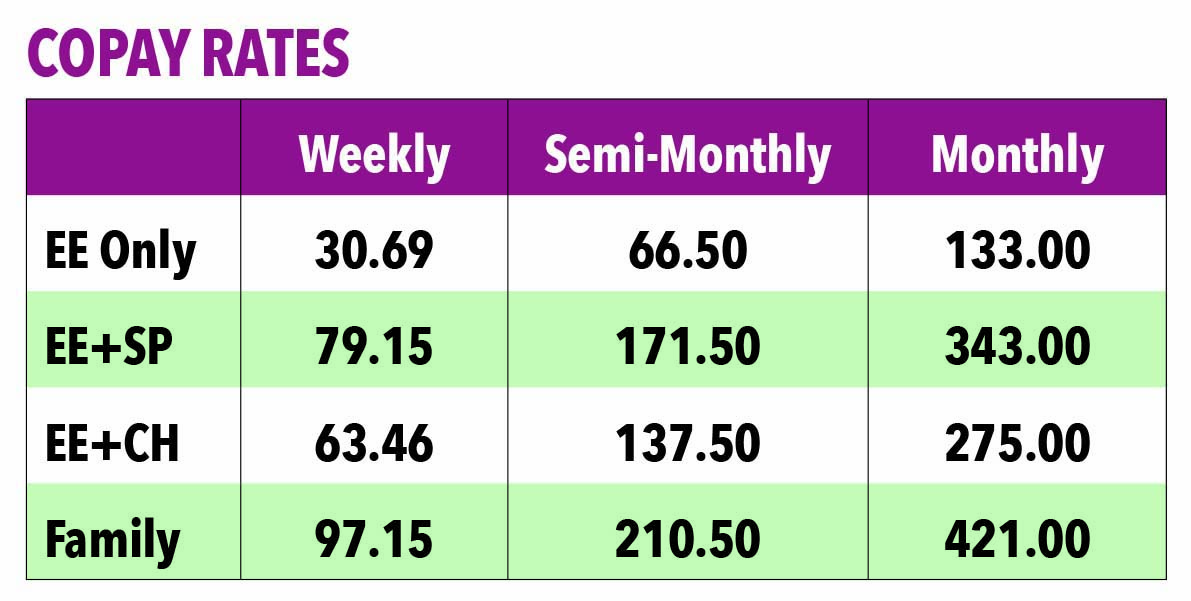
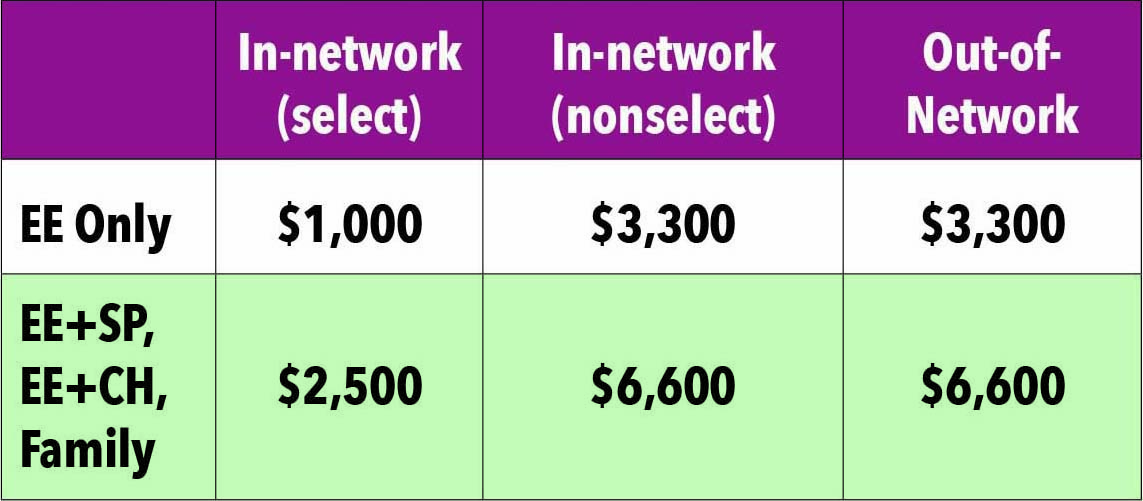
Copay Plans
| Deductibles NWGA LP, Local plus, OAP |
MMN Muskogee and Bennettsville only |
|
 |
 |
*For coverage, Spouse also refers to Common Law
New Jersey state law no longer allows state gross income tax to include pretax contribution with the exception of contributions to your 401(k) account. Federal income taxes continue to include all pretax contributions.
Medical Plan Surcharges
New enrollees to the company medical plan will be required to complete a biometric screening within 60 days of your benefit effective date to avoid a wellness surcharge. For additional details, visit the Biometrics & Coaching page.
Based on results, employees and/or covered spouses may be required to complete face-to-face, telephonic or online health coaching. Employees and covered spouses who choose not to work with a Healthy Life Team Navigator (HLN), do not make contact with their HLN or do not complete biometrics testing, will be charged an additional $28.85 per week or $125 per month as a surcharge on top of your medical plan premium.
If you enroll a spouse in the Company Medical Plan, they will be included in a spousal audit for other medical coverage. If your spouse’s employer offers insurance and you elect to cover him/her on Mohawk’s Medical Plan, you will pay an additional $125 per month in medical contributions.
*New hires and those new to the medical plan as a result of a Qualifying Life Event, please visit the Biometrics & Coaching page for details.
Surcharges:
The information below outlines ways in which medical surcharges will be applied. Keep in mind, the maximum surcharge is $57.70 per week or $250 per month in addition to your Medical plan contribution.
- $28.85/wk or $125/mo: If covered Employee does not complete a Biometric Screening when notified.
- $28.85/wk or $125/mo: If covered Spouse* does not complete a Biometric Screening when notified.
- $28.85/wk or $125/mo: If covered Employee requires Coaching based on biometric screening results and refuses to work with a health coach.
- $28.85/wk or $125/mo: If covered Spouse* requires Coaching based on biometric screening results and refuses to work with a health coach.
- $28.85/wk or $125/mo: If Spouse* enrolls in the Mohawk Medical plan and has access to other group medical coverage through their employer.
*For coverage, Spouse also refers to Common Law
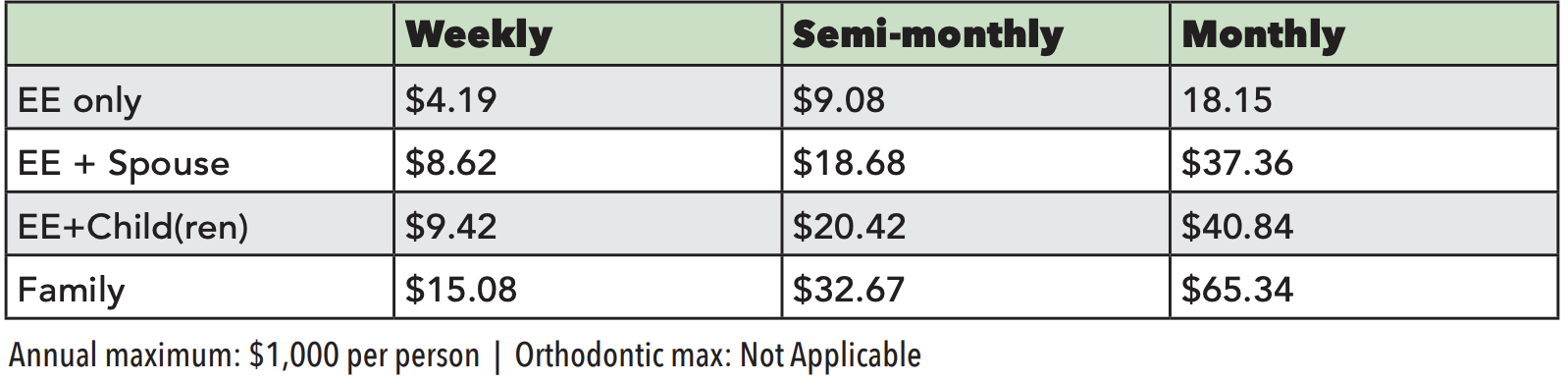
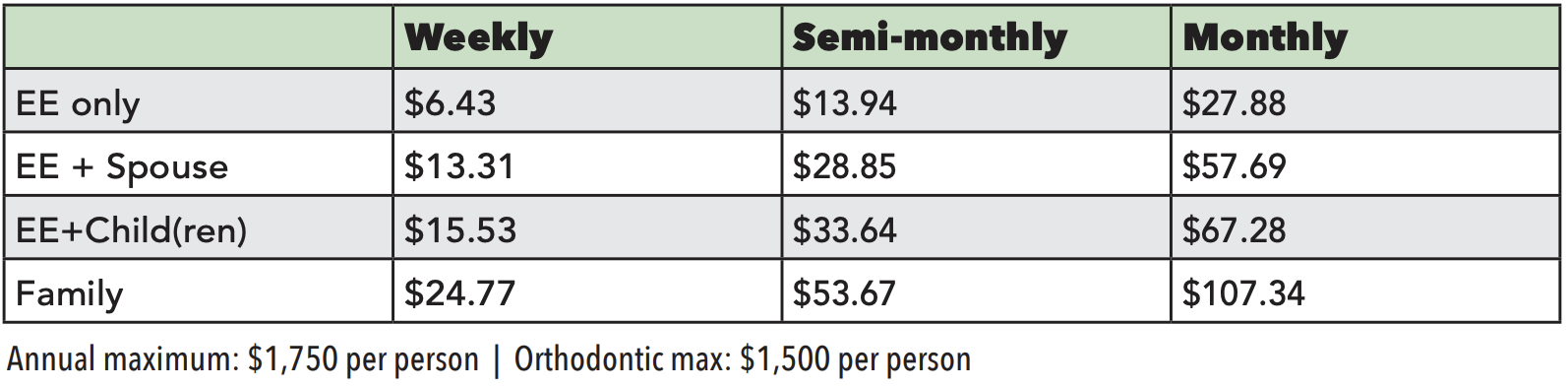
Dental Rates
Standard Mac Plan
Premium Mac Plan
Premium Access Plus Plan
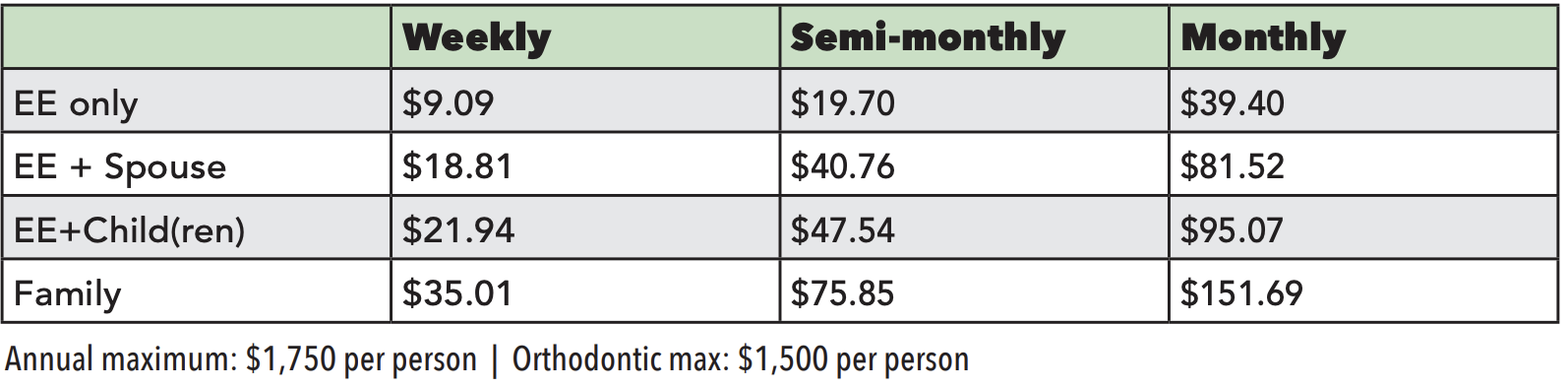
*For coverage, Spouse also refers to Common Law
Vision Plan Rates

*For coverage, Spouse also refers to Common Law
Accident Insurance
|
Coverage Level |
Weekly |
Semi- |
Monthly |
| Employee Only |
$2.61 |
$5.66 |
$11.31 |
| Employee + Spouse |
$3.75 |
$8.13 |
$16.25 |
| Employee + Child(ren) |
$5.55 |
$12.03 |
$24.05 |
| Employee + Family |
$6.69 |
$14.50 |
$28.99 |
Long-Term Disability
|
Pay Status |
Benefit |
Your Pay Period Cost |
| Hourly |
50% of base monthly salary, up to $1,000/month for 5 years |
$21.39/mo or $4.94/wk |
| Salaried, Non-exempt |
60% of base monthly salary up to $10,000/month |
($0.486 x monthly base earnings) divided by 100 divided by 2 |
| Salaried, Exempt |
60% of base monthly salary up to $10,000/month |
($0.486 x monthly base earnings) divided by 100 divided by 2 |
Payroll Deductions for Supplemental Term Life
Please note: Supplemental Life Spouse rates are based on the age of the spouse.
MONTHLY RATES for SALES AND SALARIED EMPLOYEES
Child rate - $1.28 per month, per family unit
|
Employee's/Spouse's Age |
Employee Monthly Cost per $10,000 Unit |
Employee Semi-Monthly Cost per $10,000 Unit |
Spouse Monthly Cost Per $5,000 Unit |
Spouse Semi-Monthly Cost Per $5,000 Unit |
|
Under 30 |
$0.60 |
$0.30 |
$0.30 |
$0.15 |
|
30 to 34 |
$0.80 |
$0.40 |
$0.40 |
$0.20 |
|
35 to 39 |
$0.90 |
$0.45 |
$0.45 |
$0.23 |
|
40 to 44 |
$1.44 |
$0.72 |
$0.72 |
$0.36 |
|
45 to 49 |
$2.26 |
$1.13 |
$1.13 |
$0.88 |
|
50 to 54 |
$3.80 |
$1.90 |
$1.90 |
$0.95 |
|
55 to 59 |
$6.26 |
$3.13 |
$3.13 |
$1.57 |
|
60 to 64 |
$7.82 |
$3.91 |
$3.91 |
$1.96 |
|
65 to 69 |
$13.49 |
$6.75 |
$6.75 |
$3.38 |
|
70 to 74 |
$22.00 |
$11.00 |
$11.00 |
$5.50 |
|
75 to 79 |
$33.40 |
$16.70 |
$16.70 |
$8.35 |
|
80 to 84 |
$54.10 |
$27.05 |
$27.05 |
$13.53 |
|
85 & Over |
$87.60 |
$43.80 |
$43.80 |
$21.90 |
WEEKLY RATES FOR HOURLY EMPLOYEES (Units of $10,000)
Child rate - $1.28 per month, per family unit
|
Age |
$10,000 |
$20,000 |
$30,000 |
$40,000 |
$50,000 |
$60,000 |
$70,000 |
$80,000 |
$90,000 |
$100,000 |
|
Under 30 |
$0.14 |
$0.28 |
$0.42 |
$0.55 |
$0.69 |
$0.83 |
$0.97 |
$1.11 |
$1.25 |
$1.38 |
|
30 to 34 |
$0.18 |
$0.37 |
$0.55 |
$0.74 |
$0.92 |
$1.11 |
$1.29 |
$1.48 |
$1.66 |
$1.85 |
|
35 to 39 |
$0.21 |
$0.42 |
$0.62 |
$0.83 |
$1.04 |
$1.25 |
$1.45 |
$1.66 |
$1.87 |
$2.08 |
|
40 to 44 |
$0.33 |
$0.66 |
$0.99 |
$1.33 |
$1.66 |
$1.99 |
$2.32 |
$2.65 |
$2.98 |
$3.31 |
|
45 to 49 |
$0.52 |
$1.04 |
$1.56 |
$2.08 |
$2.61 |
$3.13 |
$3.65 |
$4.17 |
$4.69 |
$5.21 |
|
50 to 54 |
$0.88 |
$1.76 |
$2.63 |
$3.51 |
$4.39 |
$5.27 |
$6.14 |
$7.02 |
$7.90 |
$8.78 |
|
55 to 59 |
$1.45 |
$2.89 |
$4.34 |
$5.78 |
$7.23 |
$8.67 |
$10.12 |
$11.56 |
$13.01 |
$14.46 |
|
60 to 64 |
$1.80 |
$3.61 |
$5.41 |
$7.22 |
$9.02 |
$10.82 |
$12.63 |
$14.43 |
$16.23 |
$18.04 |
|
65 to 69 |
$3.11 |
$6.23 |
$9.34 |
$12.46 |
$15.57 |
$18.68 |
$21.80 |
$24.91 |
$28.03 |
$31.14 |
|
70 to 74 |
$5.08 |
$10.15 |
$15.23 |
$20.31 |
$25.38 |
$30.46 |
$35.54 |
$40.61 |
$45.69 |
$50.77 |
|
75 to 79 |
$7.71 |
$15.42 |
$23.12 |
$30.83 |
$38.54 |
$46.25 |
$53.95 |
$61.66 |
$69.37 |
$77.08 |
|
80 to 84 |
$12.48 |
$24.97 |
$37.45 |
$49.94 |
$62.42 |
$74.91 |
$87.39 |
$99.88 |
$112.36 |
$124.85 |
|
85 & Over |
$20.22 |
$40.43 |
$60.65 |
$80.86 |
$101.08 |
$121.29 |
$141.51 |
$161.72 |
$181.94 |
$202.15 |
WEEKLY RATES FOR SPOUSE OF HOURLY EMPLOYEES (Units of $5,000)
Child rate - $1.28 per month, per family unit
|
Age |
$5,000 |
$10,000 |
$15,000 |
$20,000 |
$25,000 |
$30,000 |
$35,000 |
$40,000 |
$45,000 |
$50,000 |
|
Under 30 |
$0.07 |
$0.14 |
$0.21 |
$0.28 |
$0.35 |
$0.42 |
$0.48 |
$0.55 |
$0.62 |
$0.69 |
|
30 to 34 |
$0.09 |
$0.18 |
$0.28 |
$0.37 |
$0.46 |
$0.55 |
$0.65 |
$0.74 |
$0.83 |
$0.92 |
|
35 to 39 |
$0.10 |
$0.21 |
$0.31 |
$0.42 |
$0.52 |
$0.62 |
$0.73 |
$0.83 |
$0.93 |
$1.04 |
|
40 to 44 |
$0.17 |
$0.33 |
$0.50 |
$0.66 |
$0.83 |
$0.99 |
$1.16 |
$1.33 |
$1.49 |
$1.66 |
|
45 to 49 |
$0.26 |
$0.52 |
$0.78 |
$1.04 |
$1.30 |
$1.56 |
$1.82 |
$2.08 |
$2.35 |
$2.61 |
|
50 to 54 |
$0.44 |
$0.88 |
$1.32 |
$1.76 |
$2.19 |
$2.63 |
$3.07 |
$3.51 |
$3.95 |
$4.39 |
|
55 to 59 |
$0.72 |
$1.45 |
$2.17 |
$2.89 |
$3.61 |
$4.34 |
$5.06 |
$5.78 |
$6.50 |
$7.23 |
|
60 to 64 |
$0.90 |
$1.80 |
$2.71 |
$3.61 |
$4.51 |
$5.41 |
$6.31 |
$7.22 |
$8.12 |
$9.02 |
|
65 to 69 |
$1.56 |
$3.11 |
$4.67 |
$6.23 |
$7.79 |
$9.34 |
$10.90 |
$12.46 |
$14.01 |
$15.57 |
|
70 to 74 |
$2.54 |
$5.08 |
$7.61 |
$10.15 |
$12.69 |
$15.23 |
$17.77 |
$20.31 |
$22.84 |
$25.38 |
|
75 to 79 |
$3.85 |
$7.71 |
$11.56 |
$15.42 |
$19.27 |
$23.12 |
$26.98 |
$30.83 |
$34.68 |
$38.54 |
|
80 to 84 |
$6.24 |
$12.48 |
$18.73 |
$24.97 |
$31.21 |
$37.45 |
$43.70 |
$49.94 |
$56.18 |
$62.42 |
|
85 & Over |
$10.11 |
$20.22 |
$30.32 |
$40.43 |
$50.54 |
$60.65 |
$70.75 |
$80.86 |
$90.97 |
$101.08 |
Critical Illness Rates
Rates are listed in Weekly, Semi-Monthly and Monthly formats.*
NON-TOBACCO Premium - WEEKLY
| AGES | $5,000 | $10,000 | $15,000 | $20,000 | $25,000 | $30,000 | $35,000 | $40,000 | $45,000 | $50,000 |
|
18-29 |
$0.37 | $0.75 | $1.12 | $1.49 | $1.87 | $2.24 | $2.62 | $2.99 | $3.36 | $3.74 |
|
30-39 |
$0.59 | $1.19 | $1.78 | $2.37 | $2.96 | $3.56 | $4.15 | $4.74 | $5.34 | $5.93 |
|
40-49 |
$1.37 | $2.73 | $4.10 | $5.46 | $6.83 | $8.20 | $9.56 | $10.93 | $12.29 | $13.66 |
|
50-59 |
$2.35 | $4.70 | $7.05 | $9.40 | $11.76 | $14.11 | $16.46 | $18.81 | $21.16 | $23.51 |
|
60-84 |
$4.53 | $9.06 | $13.59 | $18.12 | $22.65 | $27.18 | $31.70 | $36.23 | $40.76 | $45.29 |
TOBACCO Premium - WEEKLY
| AGES | $5,000 | $10,000 | $15,000 | $20,000 | $25,000 | $30,000 | $35,000 | $40,000 | $45,000 | $50,000 |
|
18-29 |
$0.45 | $0.91 | $1.36 | $1.82 | $2.27 | $2.73 | $3.18 | $3.64 | $4.09 | $4.54 |
|
30-39 |
$0.87 | $1.74 | $2.61 | $3.48 | $4.35 | $5.22 | $6.09 | $6.96 | $7.83 | $8.70 |
|
40-49 |
$2.30 | $4.60 | $6.90 | $9.20 | $11.50 | $13.80 | $16.10 | $18.40 | $20.71 | $23.01 |
|
50-59 |
$4.68 | $9.36 | $14.05 | $18.73 | $23.41 | $28.09 | $32.77 | $37.46 | $42.14 | $46.82 |
|
60-84 |
$8.88 | $17.76 | $26.64 | $35.52 | $44.40 | $53.28 | $62.15 | $71.03 | $79.91 | $88.79 |
NON-TOBACCO Premium - SEMI-MONTHLY
| AGES | $5,000 | $10,000 | $15,000 | $20,000 | $25,000 | $30,000 | $35,000 | $40,000 | $45,000 | $50,000 |
|
18-29 |
$0.80 | $1.60 | $1.20 | $3.20 | $4.00 | $4.82 | $5.60 | $6.40 | $7.20 | $8.00 |
|
30-39 |
$1.28 | $2.55 | $1.91 | $5.10 | $6.38 | $7.65 | $8.93 | $10.20 | $11.48 | $12.75 |
|
40-49 |
$2.95 | $5.90 | $4.43 | $11.80 | $14.75 | $17.70 | $20.65 | $23.60 | $26.55 | $29.50 |
|
50-59 |
$5.10 | $10.20 | $7.65 | $20.40 | $25.50 | $30.60 | $35.70 | $40.80 | $45.90 | $51.00 |
|
60-84 |
$9.83 | $19.65 | $14.74 | $39.30 | $49.13 | $58.95 | $68.78 | $78.68 | $88.43 | $98.25 |
TOBACCO Premium - SEMI-MONTHLY
| AGES | $5,000 | $10,000 | $15,000 | $20,000 | $25,000 | $30,000 | $35,000 | $40,000 | $45,000 | $50,000 |
|
18-29 |
$0.98 | $1.95 | $2.93 | $3.90 | $4.88 | $5.85 | $6.83 | $7.80 | $8.78 | $9.75 |
|
30-39 |
$1.88 | $3.75 | $5.63 | $7.50 | $9.38 | $11.25 | $13.13 | $15.00 | $16.88 | $18.75 |
|
40-49 |
$4.98 | $9.95 | $14.93 | $19.90 | $24.88 | $29.85 | $34.83 | $39.80 | $44.78 | $49.75 |
|
50-59 |
$10.15 | $20.30 | $30.45 | $40.60 | $50.75 | $60.90 | $71.05 | $81.20 | $91.35 | $101.50 |
|
60-84 |
$19.25 | $38.50 | $57.75 | $77.00 | $96.25 | $115.50 | $134.75 | $154.00 | $173.25 | $192.50 |
NON-TOBACCO Premium - MONTHLY
| AGES | $5,000 | $10,000 | $15,000 | $20,000 | $25,000 | $30,000 | $35,000 | $40,000 | $45,000 | $50,000 |
|
18-29 |
$1.60 | $3.20 | $4.80 | $6.40 | $8.00 | $9.60 | $11.20 | $12.80 | $14.40 | $16.00 |
|
30-39 |
$2.55 | $5.10 | $7.65 | $10.20 | $12.75 | $15.30 | $17.85 | $20.40 | $22.95 | $25.50 |
|
40-49 |
$5.90 | $11.80 | $17.70 | $23.60 | $29.50 | $35.40 | $41.30 | $47.20 | $53.10 | $59.00 |
|
50-59 |
$10.20 | $20.40 | $30.60 | $40.80 | $51.00 | $61.20 | $71.40 | $81.60 | $91.80 | $102.00 |
|
60-84 |
$19.65 | $39.30 | $58.95 | $78.60 | $98.25 | $117.90 | $137.55 | $157.20 | $176.85 | $196.50 |
TOBACCO Premium - MONTHLY
| AGES | $5,000 | $10,000 | $15,000 | $20,000 | $25,000 | $30,000 | $35,000 | $40,000 | $45,000 | $50,000 |
|
18-29 |
$1.95 | $3.90 | $5.85 | $7.80 | $9.75 | $11.70 | $13.65 | $15.60 | $17.55 | $19.50 |
|
30-39 |
$3.75 | $7.50 | $11.25 | $15.00 | $18.75 | $22.50 | $26.25 | $30.00 | $33.75 | $37.50 |
|
40-49 |
$9.95 | $19.90 | $29.85 | $39.80 | $49.75 | $59.70 | $69.65 | $79.60 | $89.55 | $99.50 |
|
50-59 |
$20.30 | $40.60 | $60.90 | $81.20 | $101.50 | $121.80 | $142.10 | $162.40 | $182.70 | $203.00 |
|
60-84 |
$38.50 | $77.00 | $115.50 | $154.00 | $192.50 | $231.00 | $269.50 | $308.00 | $346.50 | $385.00 |
*All Critical Illness policies are administered by MetLife. If you had a policy with Unum in 2013, MetLife took over that policy. You may have also enrolled in additional coverage through MetLife. The advantage to retaining the policy previously held with Unum, is that the rates will not increase as you age. The rates are locked in for the life of the policy, and are not reflected in the rates contained above. If you have any questions regarding your Critical Illness coverage, please contact the Benefits Service Center at 866.481.4922.